Goodness gracious me
Those of us who grew up in foreign climes as the children of Indian expats know only too well that “everything is Indian!” However recently I was surprised to learn that a lot of this is sadly true even in my line of work as a Cardiologist.
Much of my day is involved dealing with the consequences of chronic diseases, which are brought on by the way we live. Although we can improve the symptoms and in some cases dramatically increase lifespan, we are at best palliating rather than curing. The main culprit is coronary artery disease, which can manifest itself as symptoms of chest pain on exertion (angina pectoris), chest pain at rest (acute coronary syndrome) more commonly known as a heart attack or in the worst case as sudden death.
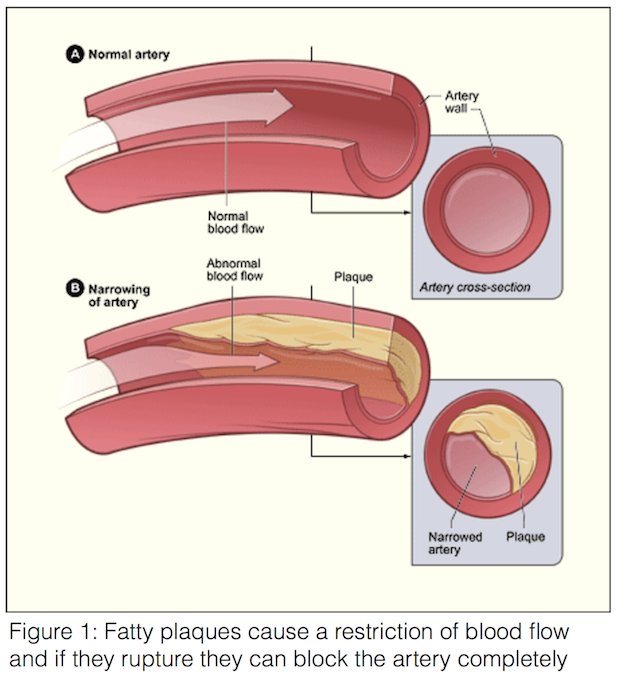
The disease process responsible for coronary artery disease is atherosclerosis, which is the furring up of arteries with fatty deposits (figure 1). Atherosclerosis has long been recognised, originally described by Leonardo da Vinci as a hardening of the arteries, which was associated with ageing. The pathogenic mechanisms that are responsible for atherosclerosis are an inflammatory reaction, which is contributed to by a number of external factors. These external factors include: smoking tobacco, high blood pressure, diabetes mellitus, high cholesterol, obesity and a sedentary lifestyle.
Unfortunately South Asians have a higher rate of coronary artery disease, are less likely to present with typical symptoms and have poorer outcomes. That is despite having a lower number of smokers, on average lower cholesterol and a lower BMI (body mass index weigh/height 2 ) than their Caucasian counterparts. This was originally in the expatriate communities who had adopted the lifestyle of the Western world, however now this is also the case in our homeland as we are projected to overtake the West making coronary artery disease very much “Indian”.
Why is this the case? The causes are multifactorial and the subject of much research, however there are a few reasons which if addressed may help stem the tide. As with everything prevention is better than attempted cure.
Lifestyle is the key to the problems we face as a modern society. Physiological adaptations which allowed our ancestors to thrive as nomadic, primitive hunter gathers are not suited to a civilisation which has mastered cultivation and mass production of food from farming. Now most of us have more than enough to eat and our health problems stem from too much. Our bodies are programmed to conserve energy and nutrients to cope with the unpredictable nature of sourcing food by our nomadic ancestors. When faced with a constant bounty rich in complex carbohydrates and sugar, the same mechanisms work against the body and contribute to what as become known as the metabolic syndrome.
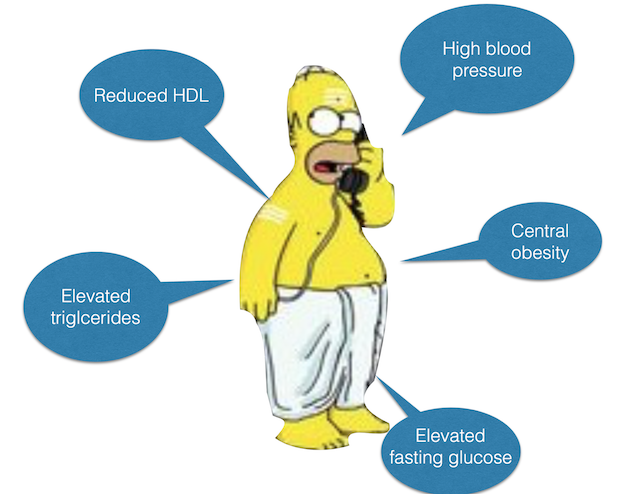
Metabolic syndrome refers to a combination of any three of the following: abdominal obesity, elevated blood pressure, high fasting glucose, elevated triglycerides (fatty acids in the blood stream) and low high density lipoproteins (good cholesterol in the blood stream). The development of metabolic syndrome increases the risk of all cardiovascular disease and in some way also explains why South Asians are more susceptible (figure 2). Although Asians have a lower BMI they tend to have a more abdominal obesity or a “paunch”. It also accepted that the normal range for BMI should be lower for South Asians, typically < 25 and that the measurement of a waist-hip ratio would be a better predictor of risk. Although South Asians have lower low-density lipoproteins (LDL or bad cholesterol) in their blood streams, they also have lower HDL, which contributes to their susceptibility to coronary artery disease. An elevated fasting blood glucose is the forerunner of diabetes and Type II diabetes is caused by insulin resistance. Insulin is the hormone responsible for processing carbohydrates and facilitates the uptake of glucose from the blood stream into cells. When the body is subjected to a constant load of carbohydrates the cells develop a reduced sensitivity to insulin and so blood glucose is elevated.
As technology makes our daily existence easier it leads to a sedentary lifestyle compared with our ancestors. A large study by Professor Salim Yusuf (originally from Kerala) showed that a reduction in our activity levels all around the world was correlated the incidence of atherosclerotic disease. Just comparing the daily routine of our grandparents to ours shows how little exercise we do going about our normal day.
So the answer is simple, eat less and do more and the problem is solved. However as many of us will know life is seldom that easy. One must be careful of simple truths, as they simply may not be true! Unfortunately the last few decades the dogma perpetuated by the world health organisation based on predominantly calorific reduction has no good supporting evidence and ignores the data, which actually supports the alternative explanations. This is why diets based on eating less calories and avoidance of fats do not necessarily lead to sustained weight loss. The only diet at that has proven health benefits is the Mediterranean diet, which is rich in olive oil and omega three fats. It has long been recognised that the intake of refined sugars are the chief culprits in the increasing prevalence of metabolic syndrome and restriction of sugar intake would have a very big impact upon the health of the population. A fact, which the sugar industry has gone to great lengths to suppress. Governmental policy which tends to lag even further behind when it comes to public health have finally cottoned on to the recommendation of public health experts with the introduction of a sugar tax. However it is too little, hopefully not too late.
There is nothing new under the sun and the basis for what I have to say comes from ancient wisdoms that have been ignored for too long. In fact in the 6th century BC Sushrata realised that the cultivation of sugar cane in India led to a pattern of disease in the rich, which he coined as “ madhumeha” or honey urine. Therefore even diabetes is “Indian”.
Trained in the allopathic traditions of the West we are very much schooled in the experimental traditions of a mechanistic approach to treating disease. This mainly focusses on treating a problem after it has arisen rather than addressing the cause and promoting prevention. What we have forgotten is a holistic approach, utilising a synergy between mind and body to maintain health and wellbeing of which diet and an active lifestyle play an important part.
Dr Badrinathan Chandrasekaran BSc MD(res) FRCP
Consultant Cardiologist
Wiltshire Cardiac Centre
Great Western Hospital
Swindon.